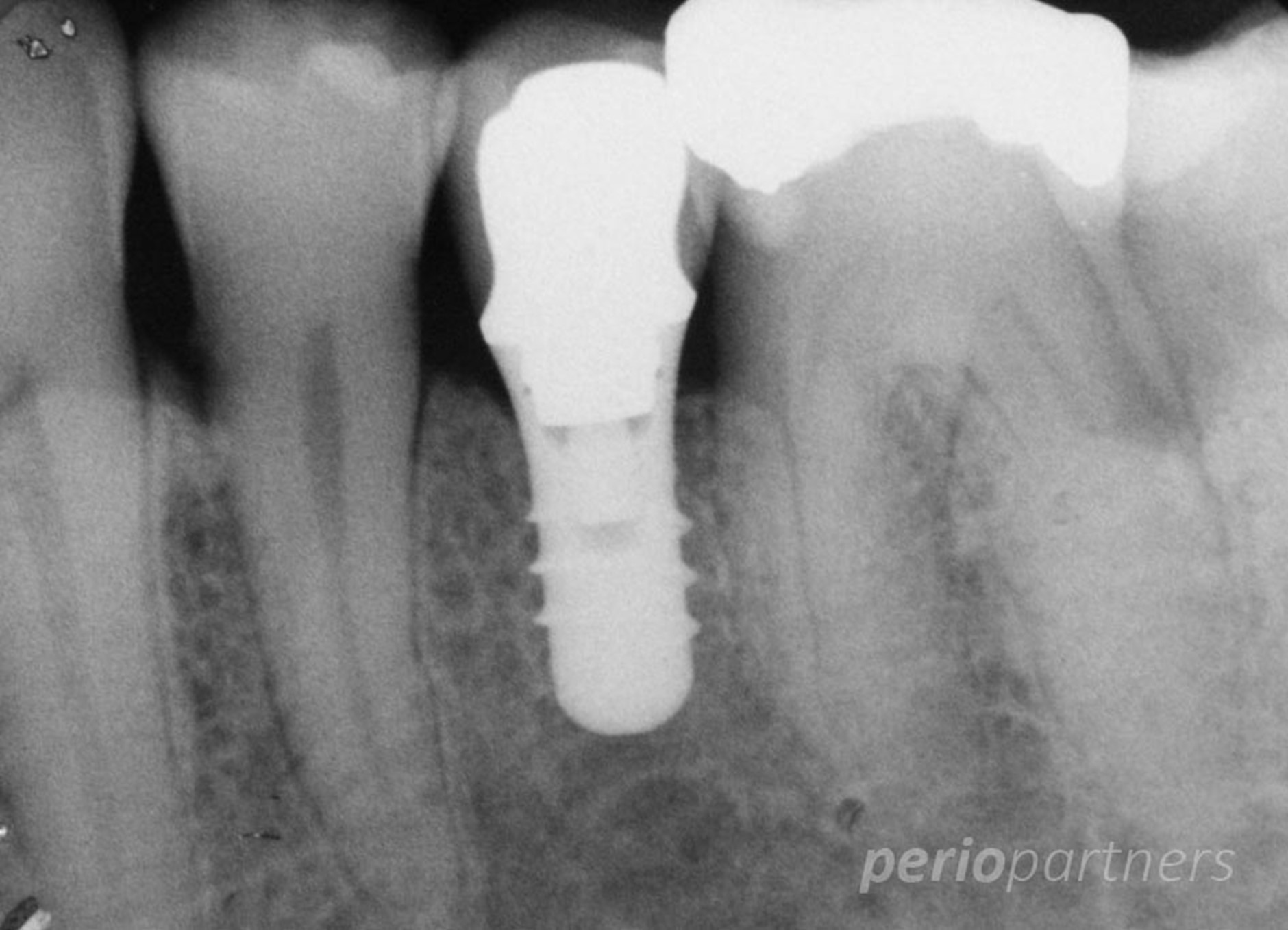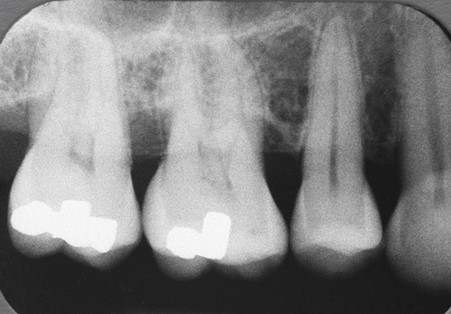
Dental implants have become the treatment of choice for the replacement of missing teeth in many situations. Dental implants can be used to support single teeth, multiple teeth (bridgework) or even full arch situations (denture or bridge). Dental implants involve the placement of an implant fixture (a medical grade titanium implant) in the jawbone, following which a tooth (crown) can be placed onto the implant. In this situation, the implant serves as the foundation of the new tooth. In most situations, the surgery for placing a single tooth implant will take less than 90 minutes. As the dental implant relies upon bone for anchorage, where the volume of bone is insufficient, bone grafting procedures may be required.
At Perio Partners, our practitioners are highly trained in the surgical placement of dental implants. We use only the most reputable implant systems and are dedicated to the follow up and long-term care of implants.